

Annual Inpatient Prospective Payment System Rule
One of the more extensive rules published each year is the Inpatient Prospective Payment System (IPPS) annual rule. Along with annual reimbursement rate increases, Medicare Severity Diagnosis Related Group (MS-DRG) weight revisions and other technical aspects of the MS-DRG reimbursements, CMS publishes a handful of data elements that impact a hospital’s reimbursement in the forthcoming federal fiscal year and future years as well. Acute care hospitals should take the following action steps upon publication of the Proposed IPPS rule. CMS published the display copy of the proposed rule on April 18, 2022.
Review Wage Index Data
A hospital’s published specific average hourly wage (AHW) and Core Based Statistical Area (CBSA) average hourly wage amounts dictate if a hospital can qualify for Medicare Geographic Reclassification qualification. Hospitals should review their published average hourly wage and ensure it reconciles to the hospital’s applicable cost report wage index survey worksheet S-3. If the hospital has requested revisions to hospital specific wage data during the past year, review to ensure requested revisions have been incorporated into the published hospital specific average hourly wage amount by CMS. AHW data is published in Table 3 annually. Supplemental Data File 8 provides detailed data reconcilable to the hospital’s applicable cost report worksheet S-3.
Hospitals MUST notify their Medicare Administrative Contractor by May 27, 2022, if revisions are required by CMS.
Review Medicare Disproportionate Share Hospital (DSH) Uncompensated Care Cost (UCC) Data
Hospital specific Uncompensated Care Cost (UCC) reimbursement is based on a hospital’s specific reported uncompensated care costs as determined on cost report worksheet S-10. A hospital’s specific UCC reimbursement Factor 3 is published on Table 18 and allows for estimate of UCC reimbursement amounts effective with discharges on or after October 1, 2022. The annual rule also includes various supplemental data files, including data file 9, DSH UCC and a hospital’s specific cost reporting year’s worksheet S-10.
Hospitals should reconcile cost report worksheet S-10 to the DSH UCC data file. If the data does not reconcile to cost report WS S-10, then the hospital must notify the Medicare Administrative Contractor immediately to ensure CMS incorporates the corrections into the final rule.
Medicare Geographic Reclassification
Published AHW data will dictate whether a hospital can qualify for Medicare Geographic Reclassification applications that will be due on September 1, 2022. Hospitals should review their ability to qualify for geographic reclassification based on the published hospital specific average hourly wage, the average hourly wage for the CBSA they are located in, and in conjunction with the Medicare Geographic Reclassification qualifying criteria.
General qualifying criteria are as follows:
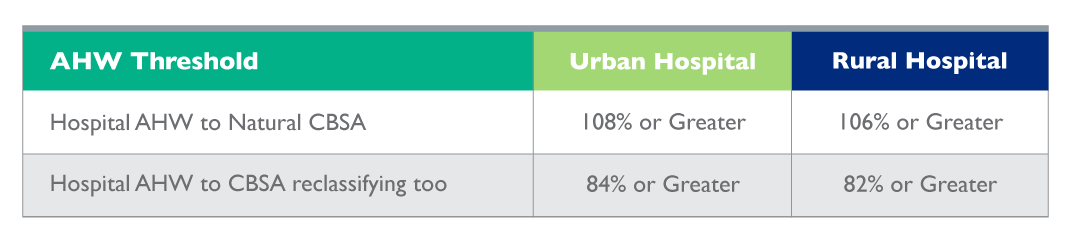
In addition, hospitals will have 45 days from publication date of the proposed rule to withdraw a prior year’s Medicare Geographic Reclassification application already approved by the Medicare Geographic Review Board. Withdrawal may be advisable if the hospital, for example, could qualify to reclassify to a different CBSA with a higher wage index.
Rural Referral Center Designation
A hospital can qualify for Rural Referral Center (RRC) designation if the hospital is located in a rural CBSA and meets specific acute care patient discharge amounts and Medicare patient case mix weights. Both the discharge and case weight thresholds are CMS determined national amounts and CMS regional amounts. For purposes of RRC qualification, CMS thresholds are set at the lower of the national discharge/case weights, or at the hospital’s region discharge/case weights.
CMS updates regional discharge and case weight thresholds annually based on prior Medicare inpatient claims submitted by acute care hospitals and publishes the data in the proposed and then final IPPS rules. Hospitals with more than 5,000 discharges should determine if they meet the published case mix index thresholds.
If the hospital is physically located in an urban CBSA, regulations found at 42 CFR Section 413.103 provide criterion for a hospital to be deemed a rural hospital for Medicare reimbursement purposes.
RRC applications and the submission process is fairly complex. Hospitals are advised to engage competent reimbursement consultants to assist in filing the application and determining if any reimbursement benefit would be obtained by the hospital with RRC designation.
For additional information, read part one of my blog here. I also encourage you to join one of my educational webinars offered through Ovation Healthcare Learning Institute.



