


These are challenging times for independent community hospitals. Some challenges, such as declining patient volumes, the rising cost of care, bad debt, and the increasing cost and complexity of compliance, are shared by larger, corporate counterparts. Others are directly related to size: the lack of economies of scale, for example, and the risk of losing key physicians and leaders to larger systems.
With fewer resources at their disposal, independent hospitals and healthcare systems must be even more focused on revenue cycle management (RCM). Here are five insights to help your hospital elevate its RCM operation to the next level.
1. Determine Your Cost to Collect (It May Be More Than You Think)
How much is it costing your hospital to collect the money it is owed? It might be more than you think, and that could be taking a big toll on the bottom line.
One important number to consider is net collection rate, a key indicator of your hospital’s effectiveness at collecting reimbursement dollars for the services it provides. According to Investopedia, it is “an effective benchmark of financial health and is key to developing a clear understanding of overall medical practice revenue cycles.”
Multiple factors could be lowering your net collection rate, including:
Do the math to determine your actual net collection rate. First divide payments received from payers and patients by total fees charged (minus approved write-offs) for the designated time period. Then multiply the result by 100 to get a percentage value, which is your net collection rate.
The industry’s target net collection rate is 96 percent, but most hospitals fall far short of that standard.
As for cost of collections, the actual number is bigger than many people realize when you factor in the total overhead, including staff salary and benefits, IT systems, training, patient access and accounting, health information management and more. Our experience is that the actual cost of collections is close to 12 percent of the revenue being collected—far more than the elusive industry ideal of 4 percent.
To lower your cost of collections and raise your net collection rate, you can have your staff master both the intricate mathematics of net collections―which includes ongoing monitoring and analysis―and the art of collecting. An alternative is to engage Amplify, an Ovation Healthcare subsidiary that has served more than 110 independent hospitals and collected over $370 million, to ‘rebadge’ your hospital’s collection staff, taking them off your hospital’s payroll and onto ours, significantly lowering your cost of collections.
An excellent example is an Amplify client that is a 25-bed critical access hospital in northwestern South Carolina. In one year, Amplify increased collections at the hospital by $1.1M above what they collected in the prior year. This is in addition to a volume increase of 14.9 percent.
2. Accelerate Cash on Flat Revenue, Reducing DNFB
DNFB is not a favored abbreviation in any hospital collections department. Short for ‘discharged not final billed,’ it refers to the ratio of accounts held for billing for any of various reasons―mostly related to invalid, inaccurate, missing or delayed coding or data.
Coding backlogs. Codes that don’t correspond to charges. Invalid codes. Missing or incorrect patient data. Inaccurate payer designator coding. All these issues could lead to an account’s DNFB status. And inaccuracy is expensive: Lack of physician documentation and other information gaps not only can delay reimbursements but also can bring financial penalties from government health programs.
If a hospital is having difficulty managing cash flow, it may be unable to adequately sustain its daily operations and provide the best possible care for its patients.
What’s needed is a way to speed up reimbursements and improve cash flow without sacrificing coding accuracy. That means fixing the front end of the revenue cycle.
Muenster Memorial Hospital in Cooke County, Texas, which was struggling with a high DNFB as well as excessive accounts receivable (AR), used Amplify’s proprietary tools and experienced staff to provide training and mentoring for ongoing improvement and success.
The Amplify process includes:
The result for Muenster Memorial was a DNFB improvement from 29 days of gross revenue to five days, an 83 percent reduction. In addition, the hospital’s accounts receivable (AR) was reduced over 90 days from $1,179,000 to $474,000. The AR cleanup generated more than $700,000 in cash collections, while the DNFB reduction accelerated an additional $300,000, bringing the 18-bed critical access hospital more than $1 million in previously uncollected cash.
Through this process, Muenster Memorial also gained tools for long-term success: an improved organizational structure, the identification of staff deficits, and a training program that addressed working procedures and standards―leading to increased staff confidence and performance.
3. Get in Line With Reimbursement Changes
New changes to federal reimbursement regulations could affect independent community hospitals. A lack of attention to them could result in money left on the table—or even hinder their ability to serve their communities.
You could be missing out on the opportunity to receive additional reimbursement as either a Sole Community Hospital (SCH) or a Medicare Dependent Hospital (MDH). Both of these designations were created by legislation to address access-to-care issues and maintain the financial viability of rural hospitals.
Meanwhile, pending rules designed to protect consumers from what is known as ‘surprise billing’ could have unintended consequences.
Here’s a quick overview of the most relevant highlights from these developments:
SCH and MDH Designation
A hospital can become an SCH or an MDH but not both. Qualification as an SCH can be based on its isolated location (urban or rural, at least 35 miles from other ‘like’ hospitals); by definition, distance from nearest “like” hospital excludes Critical Access Hospitals. Hospitals located in rural areas within 25 to 35 miles may qualify if certain market share or travel time thresholds are satisfied.
Basic criteria for MDH designation are a rural location, 100 or fewer acute care beds and Medicare utilization of at least 60 percent as reported on two of the three most recent final settled Medicare Cost Reports.
A pressing reimbursement opportunity for SCHs and MDHs is the Decrease in Patient Discharges Reimbursement Adjustment. SCHs/MDHs that experience a five percent decrease in hospital discharges can qualify for an additional reimbursement amount if federal inpatient reimbursements are less than Medicare inpatient costs as determined through the Medicare Cost Report. With many US hospitals experiencing a decrease in discharges due COVID19 in their 2020 and 2021 fiscal years, multiple SCHs/MDHs may qualify for the Decrease in Patient Discharges Reimbursement Payment.
Applications must be filed within 180 days of the final settlement of the Medicare Cost Report. Applications can be filed after the cost report is filed and Medicare Administrative Contractors will make a tentative payment for qualifying SCHs/MDHs
Surprise Billing
The Biden administration has published Interim Final Regulations implementing the Surprise Billing Act of 2021, which was included in the Consolidated Appropriation Act of 2021, enacted on December 27, 2020. The Surprise Billing Act and Interim Final regulations are specifically consumer protections established to limit patients’ out-of-pocket costs when receiving services at hospitals.
According to regulations published concurrently by multiple federal agencies including the Centers for Medicare and Medicaid Services, the consumer protections that took effect January 1, 2022:
- Ban balance billing in all cases.
- Ban surprise billing for emergency services, including air ambulance services, requiring such services to be billed at in-network prices.
- Ban high out-of-network cost-sharing for emergency medical services. Cost sharing will always be at in-network rates.
- Post emergency and non-emergency services cost sharing will be at in-network rates as well unless providers provide specific Surprise Billing Notices to patients and such patient provides a signed consent for out-of-network cost sharing.
- Requires out-of-pocket estimates to uninsured patients.
- Requires out-of-pocket estimates for insured patients. This is currently on hold until insurance carriers and providers develop appropriate infrastructure.
- Remove patients from billing disputes between providers and insurers with creation of Independent Resolution Dispute entities.
Surprise Billing regulation could have unintended consequences for patients, the National Rural Health Association (NRHA) has warned. NRHA is seeking modifications to avoid potential negative impacts on patients. Those include rules relating to emergency air medical services, which it says could leave patients without access to care in the most rural, underserved communities; and provisions subjecting rural providers to “overly burdensome” price transparency regulations, which it says could force struggling rural providers to devote more staff time to fulfilling unnecessary regulations.
4. Navigate Compliance and Operationalize Change
Compliance with the range of new and updated healthcare-related laws, rules and regulations is increasingly costly and complex, especially for independent hospitals and healthcare systems.
An effective compliance program leverages available technology and resources to prevent, detect and respond to fraud, waste and abuse. Noncompliance in some cases can lead to fines or other penalties, as well as damage to a hospital’s reputation for ethical behavior.
Ensuring that your program meets the expectations of the Department of Justice and the Office of Inspector General for Health and Human Services in complying with relevant federal healthcare laws and regulations requires great attention to detail. It also requires an actively promoted culture of compliance that engages your stakeholders and is focused on ethical behavior.
An experienced compliance solutions team can help you with assessment of existing policies, procedures, tools and forms; evaluation of real-time on-site corrective assistance; assessment of implementation and educational programs; and more. Specific services include:
- Program effectiveness evaluations, risk assessments and mitigation,
- Compliance officer training and oversight,
- Education and training,
- Monitoring and auditing,
- Enforcement and discipline,
- Code of conduct, policies and procedures,
- Reporting and communication,
- Response and corrective action, and
- Physician arrangement reviews
These services can help your hospital or system operationalize change, incorporating it into the daily activities of frontline staff and others so that ethical and compliant behavior is second nature to everything they do.
5. RCM Solutions Aren’t One Size Fits All―Customize What Works for You
For independent community hospitals and healthcare systems, revenue cycle management can be intensified by the absence of a parent corporation that can ease the load by providing access to shared resources, deeper discounts on supplies, economies of scale, negotiating power, financing and more.
Today’s top RCM challenges include:
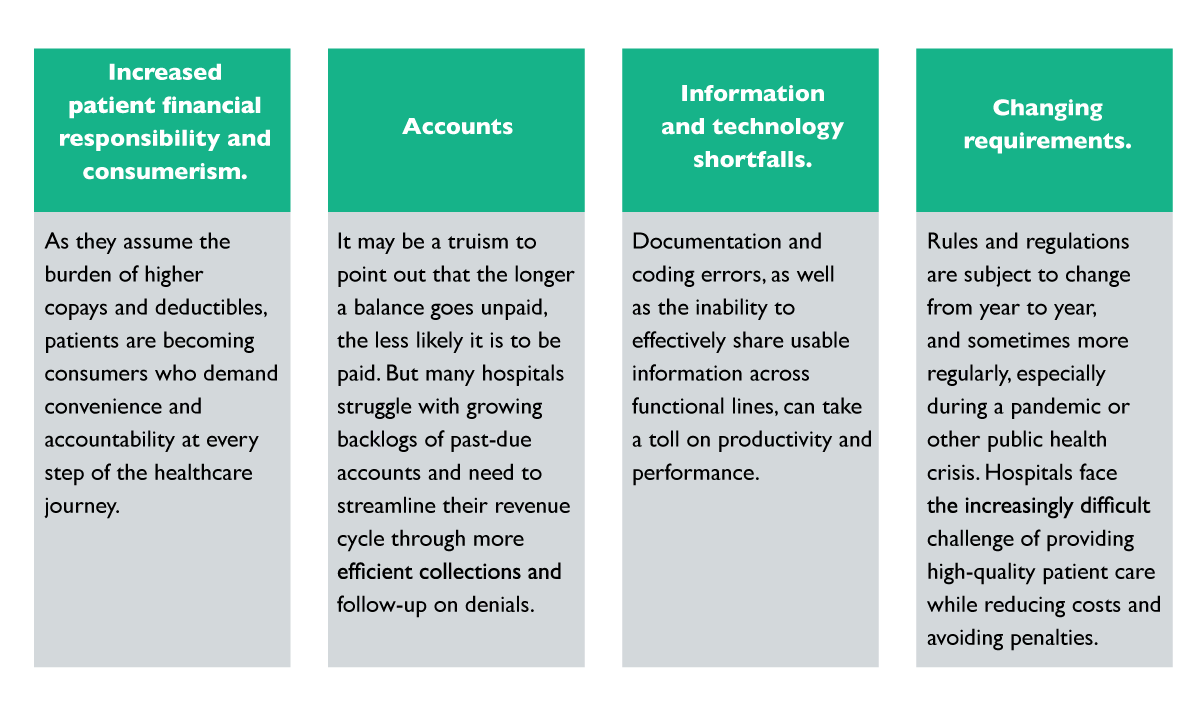
Within its community, each hospital also has its own unique set of demands. That means solutions are far from one size fits all.
Reasons to Engage
Reasons to engage an RCM vendor also are likely to vary from hospital to hospital. Needs could include:
- Knowledge of best practices and leadership through change. The past experiences and current practices of those who have been through what you’re facing now can help your organization prepare for the inevitable change through communication, collaboration and commitment.
- Up-to-date education on changes in rules and regulations. Federal rules, regulations and guidelines are frequently changing. Neglecting these changes could be costly to your bottom line, as well as to your legal standing and public reputation.
- Assistance with department structure. Old structures often require modification to meet current needs. Are artificial divisions in your organization hindering information sharing, teamwork or patient experience?
- Assistance determining appropriate metrics and tracking capabilities. How you measure can be just as important as what you measure. When tracking the progress of your hospital, you want the data you generate to be specific, measurable, achievable, relevant and time-bound.
- Evaluation or audit. Whether the area of concern is the current state of staffing, data capture, leadership, length-of-stay or level-of-care impact, trustworthy information is essential to smart decision making.
Customization and Flexibility
Ovation Healthcare’s shared services model for hospital management and consulting recognizes your need for customization and flexibility. All the above services are available, along with others, with work tailored to your unique needs. That flexibility extends not only to scheduling, but also to educational offerings for leadership.



